All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a Healthcare Professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub uses cookies on this website. They help us give you the best online experience. By continuing to use our website without changing your cookie settings, you agree to our use of cookies in accordance with our updated Cookie Policy
Introducing

Now you can personalise
your Lymphoma Hub experience!
Bookmark content to read later
Select your specific areas of interest
View content recommended for you
Find out moreThe Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.









AACR 2017 | Poster 3150/10 – PLCG2 C2-domain mutations co-occur with BTK and PLCG2 resistance mutations in Chronic Lymphocytic Leukemia undergoing ibrutinib therapy
Bookmark this article
At the American Association for Cancer Research (AACR) annual meeting in Washington, DC, USA, on Tuesday 4th April, a poster session titled “Molecular Targeted Therapies 1” took place.
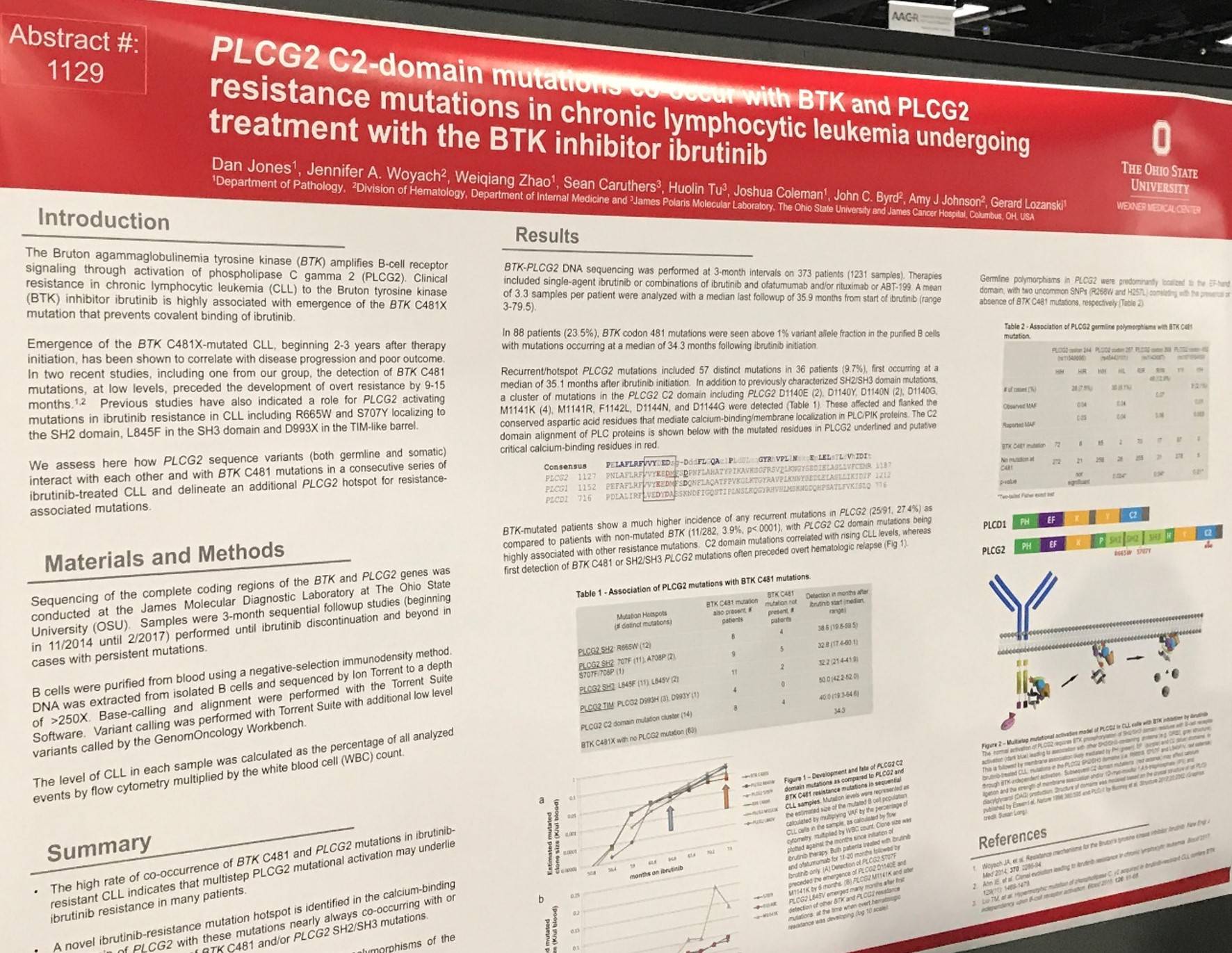
One of the posters on display (3150 / 10) was titled “PLCG2 C2-domain mutations co-occur with BTK and PLCG2 resistance mutations in chronic lymphocytic leukemia undergoing treatment with the BTK inhibitor ibrutinib” by Dan Jones from The Ohio State University, Columbus, OH, and colleagues.
The group analyzed all peripheral blood samples from CLL patients, with suitable depth of sequencing coverage, submitted to the Ohio State University James Polaris Molecular Laboratory.
Key Highlights:
- BTK-PLCG2 DNA sequencing carried out at 3-month intervals on 373 patients (1,231 samples)
- Treatments included ibrutinib monotherapy, or ibrutinib combined with ofatumumab and/or rituximab or venetoclax
- BTK codon 481 mutations observed above 1% variant allele fraction = 23.5% (88) patients
- Median time after ibrutinib initiation to BTK codon 481 mutation = 34.3 months
- Fifty-seven distinct recurrent/hotspot PLCG2 mutations observed in 9.7% (36) patients
- Median time after ibrutinib initiation to PLCG2 mutation = 35.1 months
- Formerly reported mutations in SH2/SH3 domains of PLCG2 were found: R665W, S707F, A708P, and L845F
- Novel mutations in the PLCG2 C2 domain were observed affecting codons 1140–1144, which code for the highly conserved aspartic acid residues that bind calcium and mediate membrane localization in other C2-domain containing proteins
- Patients harboring BTK mutations had a much higher incidence of recurrent mutations in PLCG2 (25/91, 27.4%) versus patients with wild-type BTK (11/282, 3.9%; P < 0.0001)
- PLCG2 C2 domain mutations were highly associated with other resistance mutations
- PLCG2 C2 domain mutations correlated with increasing CLL levels (clone size), whereas first identification of BTK codon 481 or SH2/SH3 PLCG2 mutations frequently came before hematologic relapse
- PLCG2 germline polymorphisms were mainly located to the EF-hand domain; R268W and H257L were two uncommon single nucleotide polymorphisms reported, correlating with presence or absence of BTK codon 481 mutations, respectively
The poster was summarized by stating that a high rate of co-occurrence of BTK codon 481 and PLCG2 mutations was found in samples from CLL patients unresponsive to ibrutinib. The group hypothesize that “multistep PLCG2 mutational activity may underlie resistance in many patients.” The authors also concluded by stating that they identified a novel mutation hotspot – the PLCG2 C2 domain – which often co-occurs with or after BTK codon 481 and/or PLCG2 SH2/SH3 mutations. Finally, it was also found that BTK mutations segregate with different PLCG2 germline polymorphisms.
- Jones D. et al. PLCG2 C2-domain mutations co-occur with BTK and PLCG2 resistance mutations in chronic lymphocytic leukemia undergoing treatment with the BTK inhibitor ibrutinib [Poster]. In: Proceedings of the 107th Annual Meeting of the American Association for Cancer Research; 2017 Apr 1-5; Washington, DC. Philadelphia (PA): AACR; 2017. Poster nr [3150 / 10].

Understanding your specialty helps us to deliver the most relevant and engaging content.
Please spare a moment to share yours.
Please select or type your specialty
 Thank you
Thank youRelated articles
Newsletter
Subscribe to get the best content related to lymphoma & CLL delivered to your inbox