All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a Healthcare Professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The Lymphoma Hub uses cookies on this website. They help us give you the best online experience. By continuing to use our website without changing your cookie settings, you agree to our use of cookies in accordance with our updated Cookie Policy
Introducing

Now you can personalise
your Lymphoma Hub experience!
Bookmark content to read later
Select your specific areas of interest
View content recommended for you
Find out moreThe Lymphoma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Lymphoma Hub cannot guarantee the accuracy of translated content. The Lymphoma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.









ASH 2016 | Educational Session: Long-Term Risk of Second Malignancy and Cardiovascular Disease After Hodgkin Lymphoma Treatment
Bookmark this article
On Saturday 3rd December, during the 58th Annual Meeting & Exposition of the American Society of Hematology (ASH), in San Diego, CA, an educational session took place between 9.30am–11.00am, titled “Hodgkin Lymphoma: Treatment Today and the Challenge for Tomorrow.” This session was Chaired by Andrew Lister, MD, of Barts Cancer Institute, London, UK, and focused on how the outcome of patients with HL in 2016 can be improved, beyond that achieved in the last 50 years, with combination chemotherapy and extended-field megavoltage radiotherapy.
“Long-Term Risk of Second Malignancy and Cardiovascular Disease After Hodgkin Lymphoma Treatment” was the last talk during this session, and was presented by Flora E. Van Leeuwen, PhD, from the Netherlands Cancer Institute, Amsterdam, Netherlands.
Second Cancers
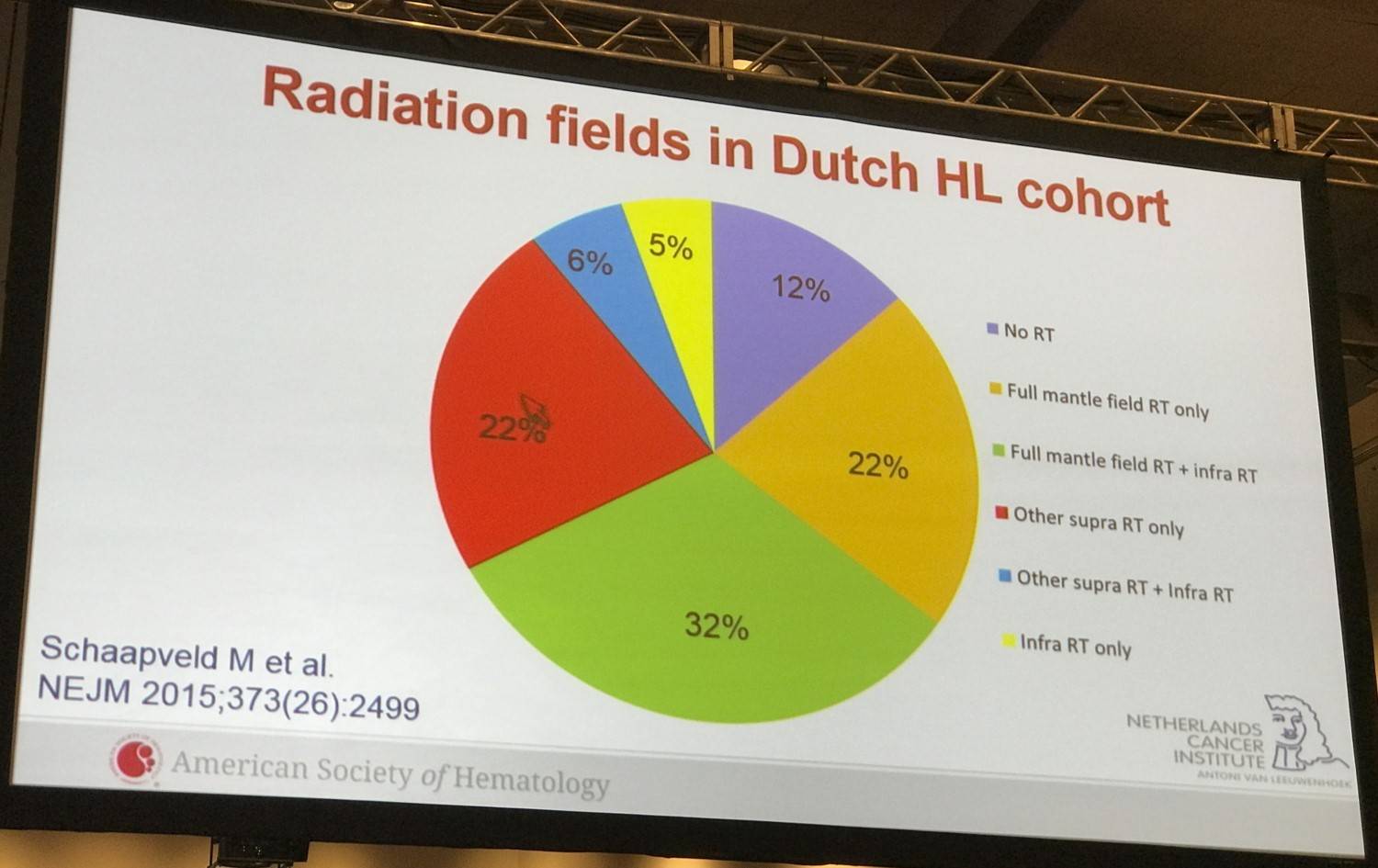
Van Leeuwen began the talk by exploring a study by Schaapveld M. et al., published in 2015, which investigated the long-term risk of secondary cancers and changes in risk over time in a large cohort of survivors of HL in the Netherlands. These patients had been treated between 1965 and 2000 and had detailed information on primary and relapse treatment and complete follow-up for second cancers. 3,905 patients were included from 6 (University Medical) Cancer Centers and 41 community hospitals. The median age at HL diagnosis was 28.6 years (range 15–50 years) and 43% patients were female. Median follow-up time was 19 years (range 5–47 years) and was carried out through medical charts, letter to GPs and linkage with Dutch pathology registry and the Netherlands Cancer Registry. Radiation therapy alone, chemotherapy alone, and radiation and chemotherapy was received by 27.3%, 12.1%, and 60.5% of patients, respectively.
During follow-up:
- 1,055 second cancers were diagnosed in 908 patients; three cancers developed in 130 patients, and four developed in 17
- The risk of a second cancer among patients treated for HL was higher than the incidence of cancer in the general population (Standardized Incidence Ratios [SIR], 4.6; 95% CI, 4.3–4.9), resulting in 121.8 excess cancers per 10,000 person-years
When estimating the cumulative incidence of secondary malignancies, death was treated as a competing risk. Trends over time were evaluated in competing-risk models, adjusting for sex, age, and smoking status when appropriate.
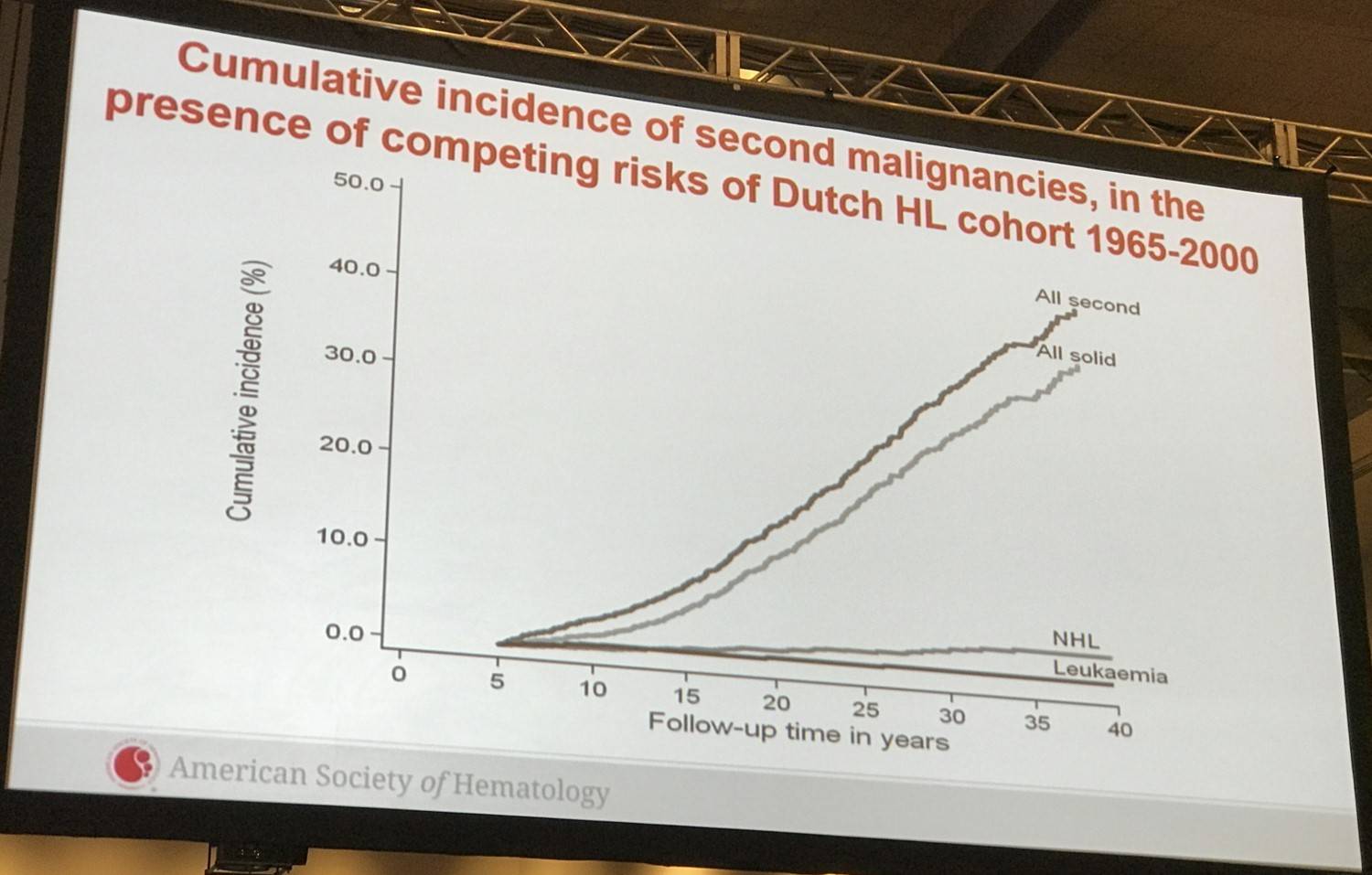
- At 40 years, the cumulative incidence was 48.5% (95% CI, 45.4–51.5) compared with the expected cumulative incidence of 19.0% in the general population
- The cumulative incidence of any second cancer was lower among patients treated from 1989–2000 than those treated from 1965–1976 (sub-distribution HR, 0.79; 95% CI, 0.65–0.95; P=0.02)
The expected and observed numbers of second cancers were used in standard methods to calculate the SIRs and the Absolute Excess Risk (AER) per 10,000 person-years.
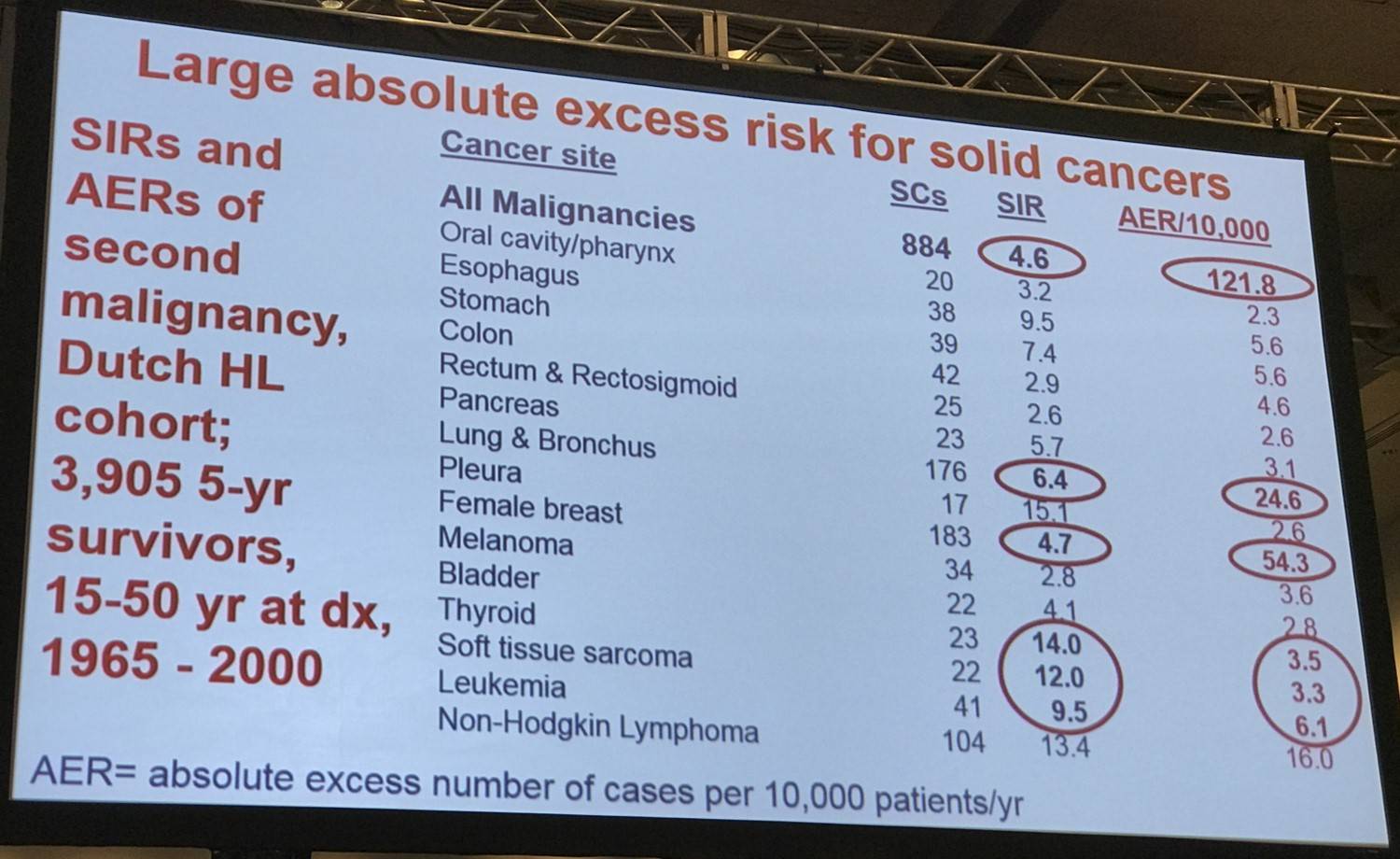
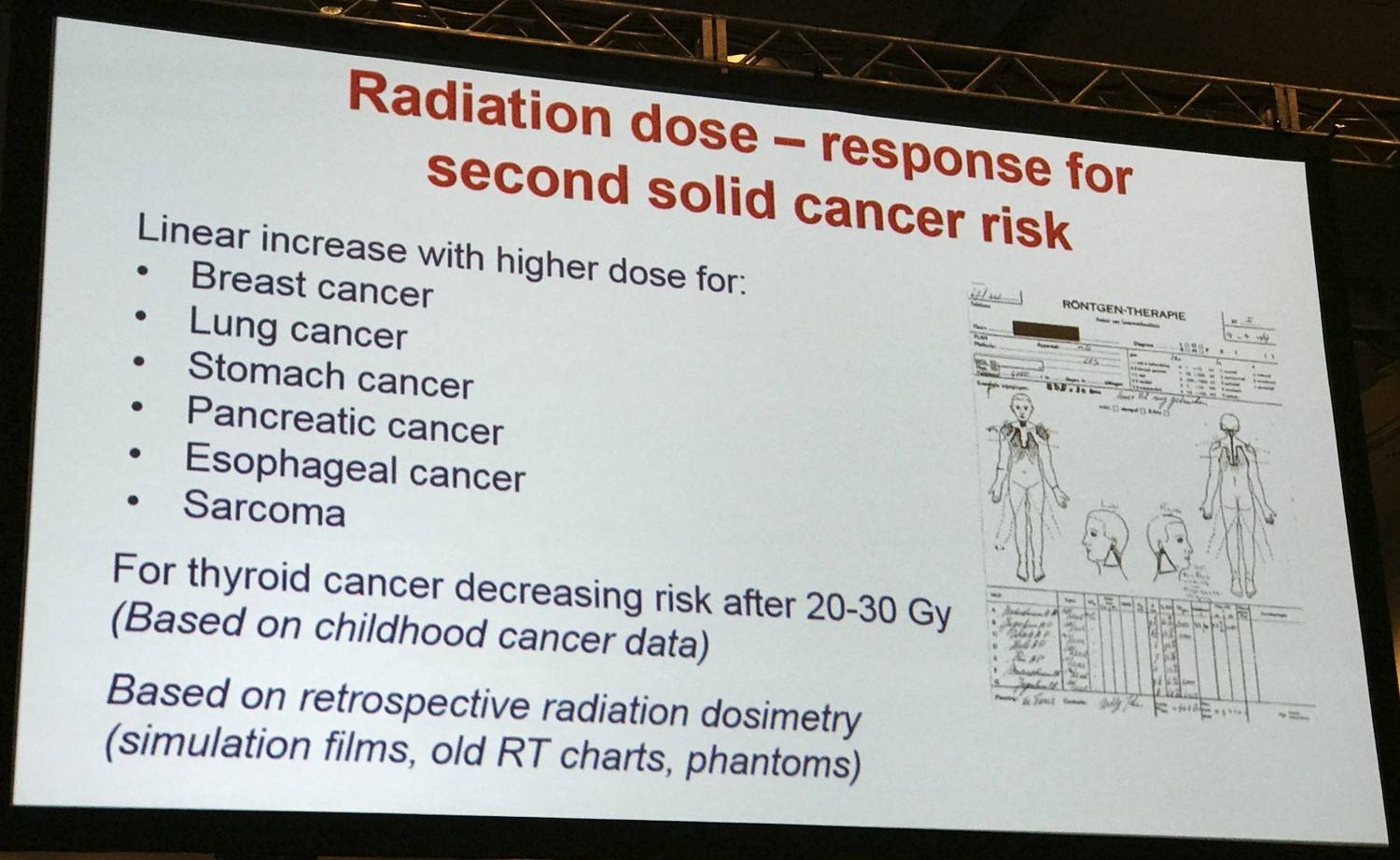
- The significantly higher relative risks of thyroid cancer, mesothelioma, and soft-tissue sarcoma were associated with low absolute risks (30-year cumulative incidence, 0.8%, 0.6%, and 0.7%, respectively), due to low background risks in the population
- AER of breast cancer among women = 54.3 cases per 10,000 person-years; 40.5% of the excess risk of any second cancer (134.0 cases per 10,000 person-years) among women in the cohort
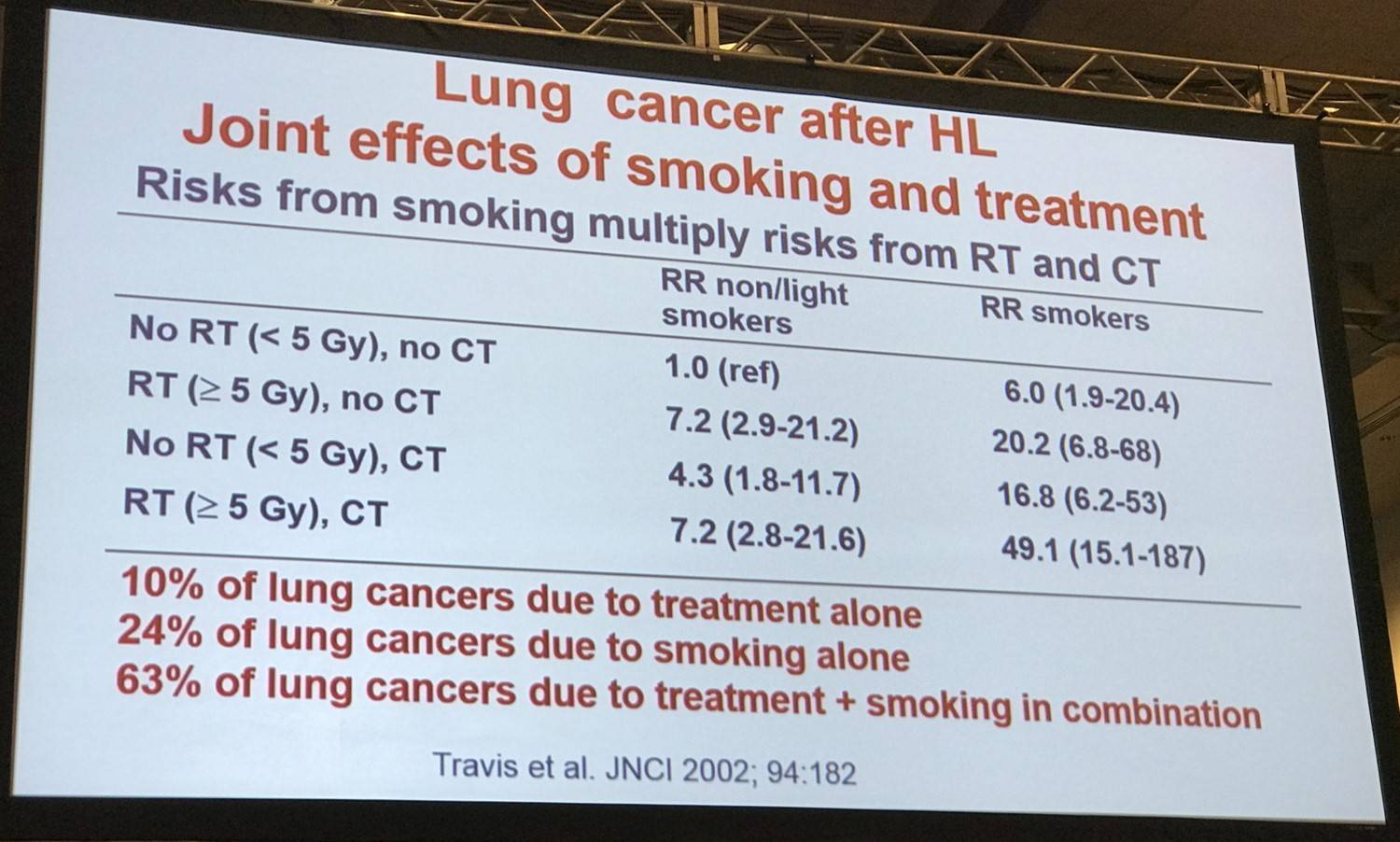
- Lung cancer was the next most common, AER = 24.6 cases per 10,000 person-years; 20.2% of the excess risk in the cohort
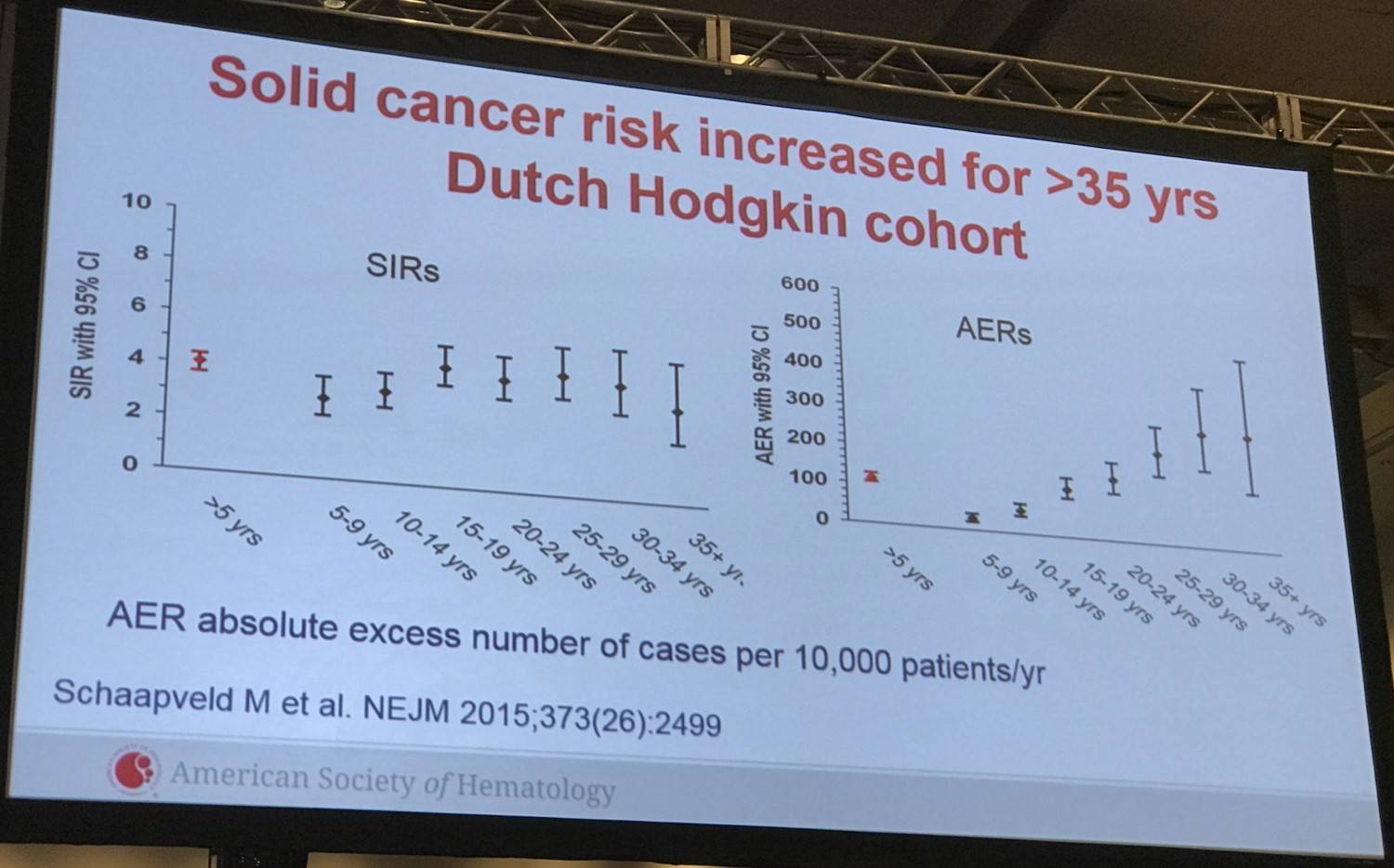
- The SIR for any second cancer remained high for at least 35 years after the start of HL treatment (SIR for ≥35 years, 3.9; 95% CI, 2.8–5.4) whereas the AER increased steadily over time (P<0.001)
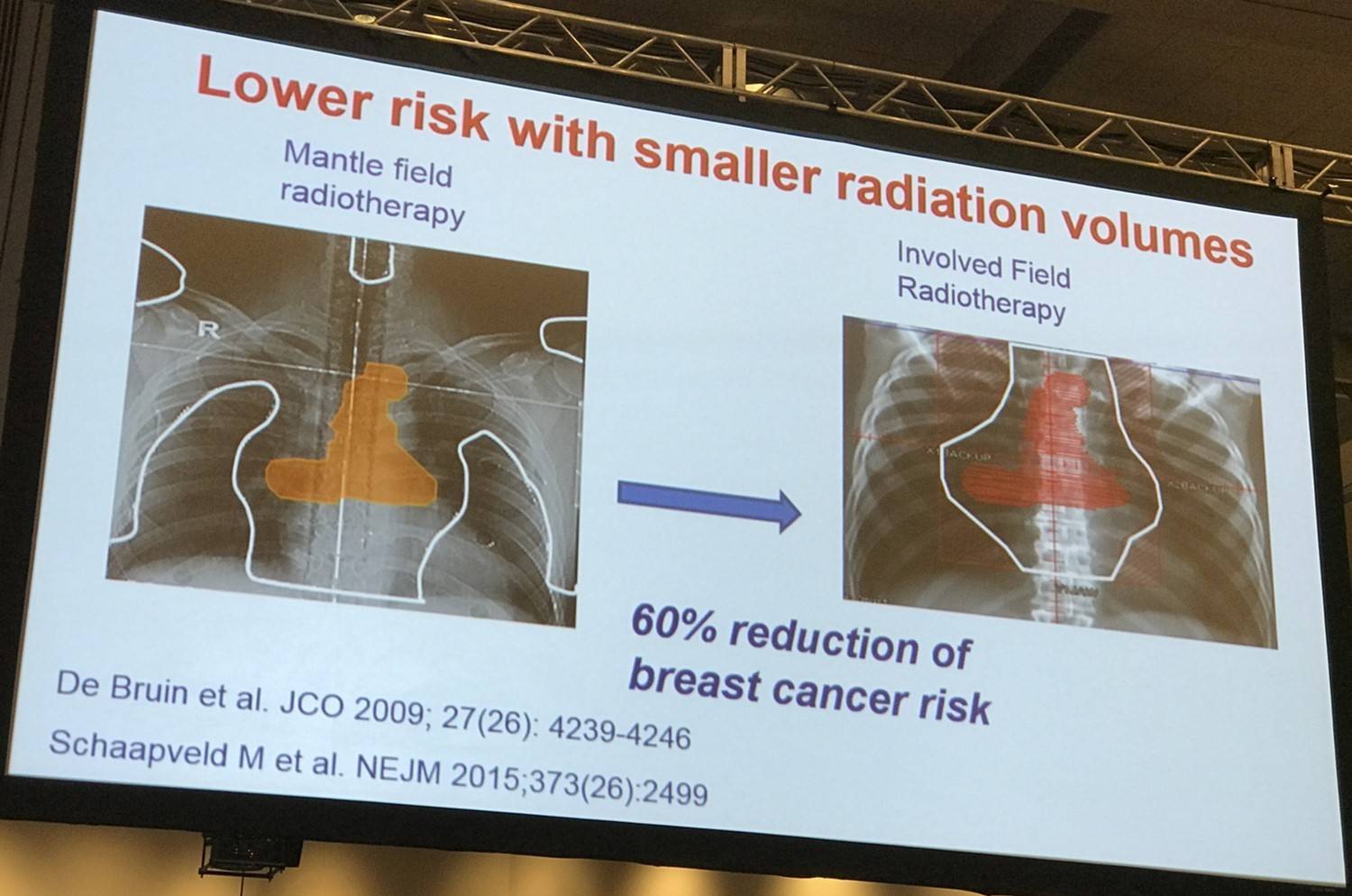
- Patients who received supradiaphragmatic field radiotherapy not including the axilla had a lower risk of secondary solid cancer than patients who received complete mantle-field radiotherapy (HR, 0.63; 95% CI, 0.49–0.83)
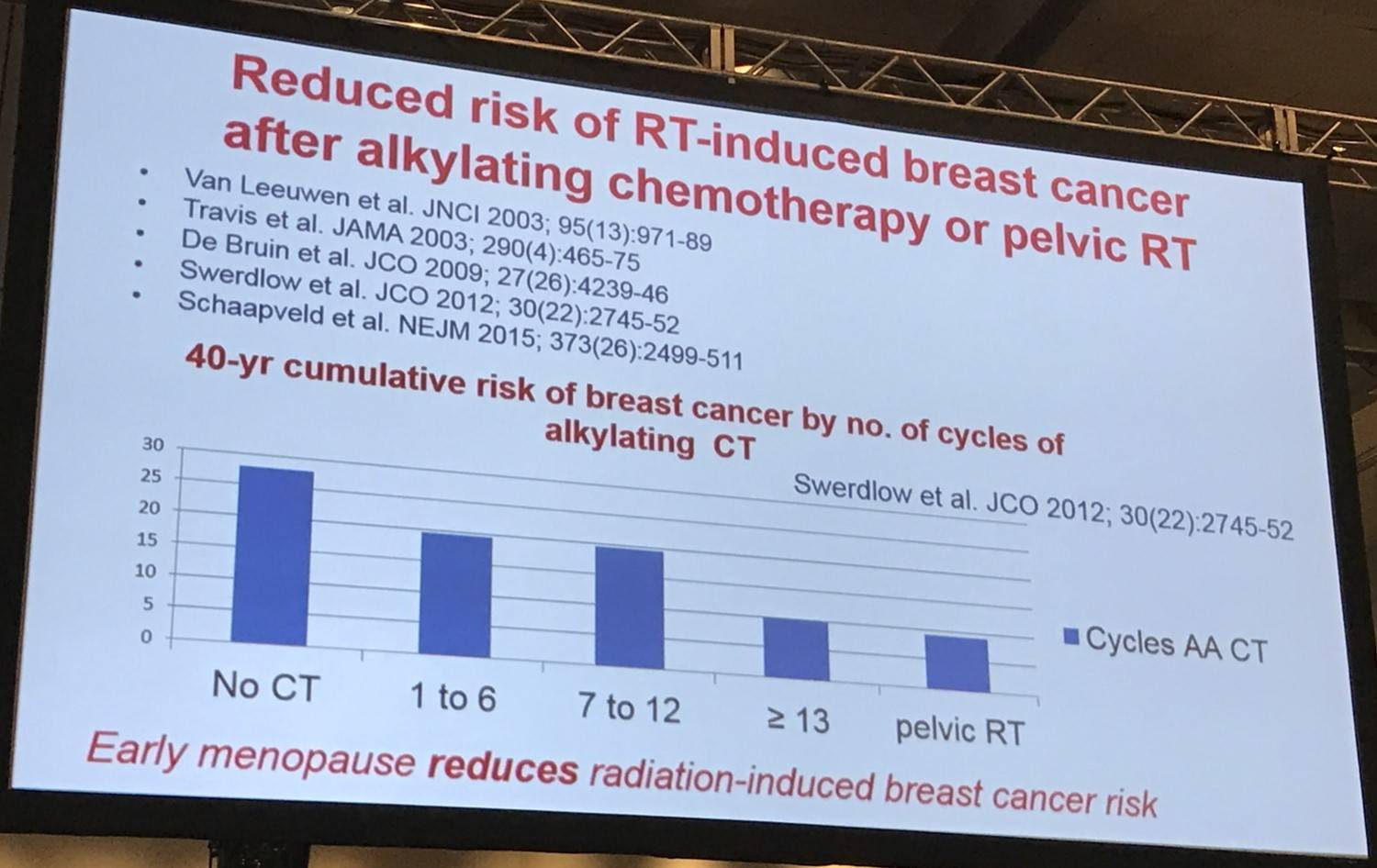
- The risk of breast cancer was lower with higher cumulative procarbazine doses (HR for a cumulative procarbazine dose of ≥4.3g/m2 vs no chemotherapy, 0.57; 95% CI, 0.39–0.84; P=0.002)
- Patients treated with mantle-field irradiation had a risk of lung cancer that was similar to the risk among those treated with less-extensive supradiaphragmatic field irradiation (HR, 1.04; P=0.84)
Prof. Van Leeuwen then outlined the risk of t-AML/MDS after HL by sharing data from German Hodgkin Study Group trials from 1993 to 2009, published by Eichenauer et al. in 2014. They found 106 t-AML/MDS cases occurred in 11,952 patients and median time to t-AML/MDS was 31 months.
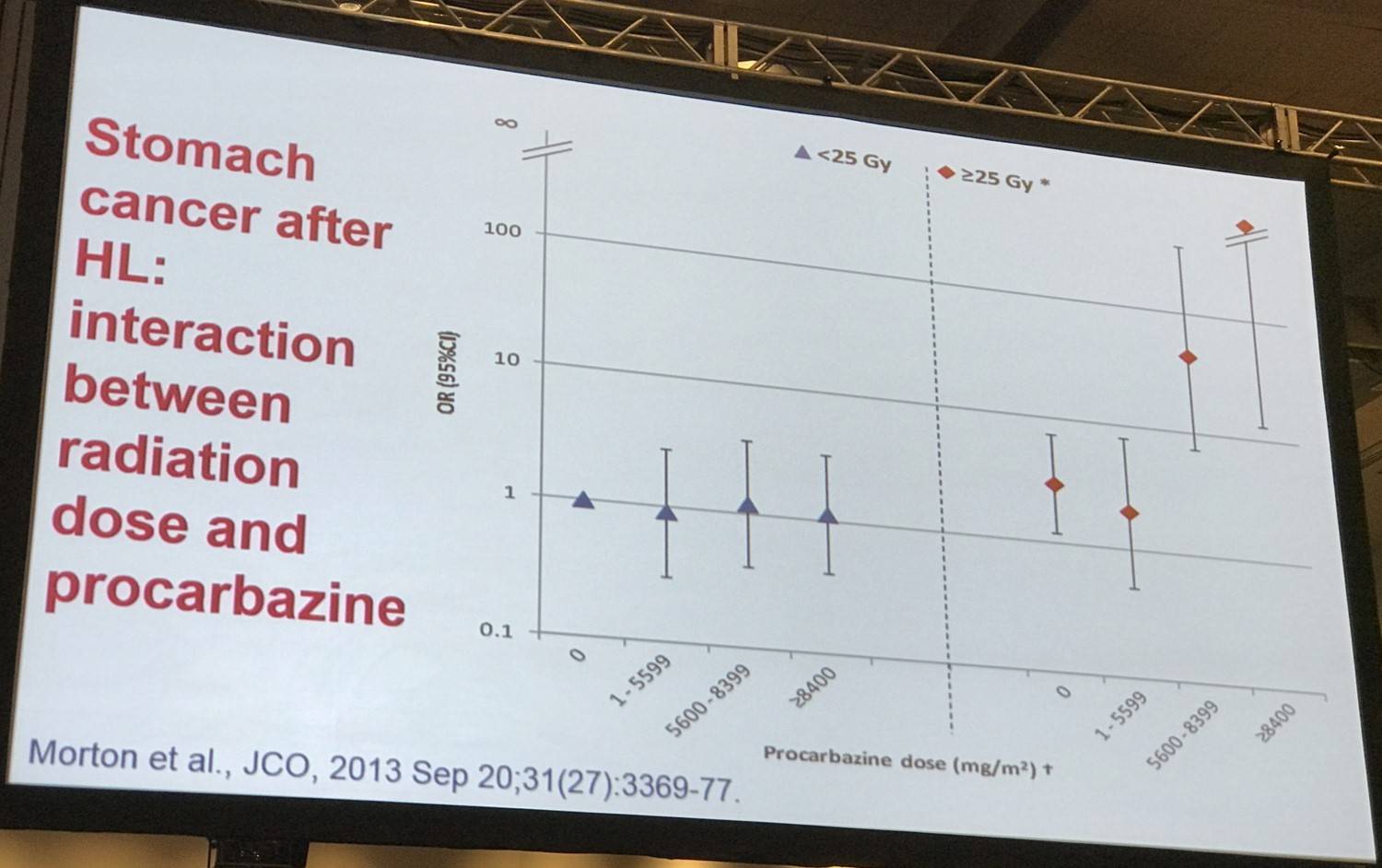
This was followed by outlining data published by Morton et al. in the Journal of Clinical Oncology in 2013.
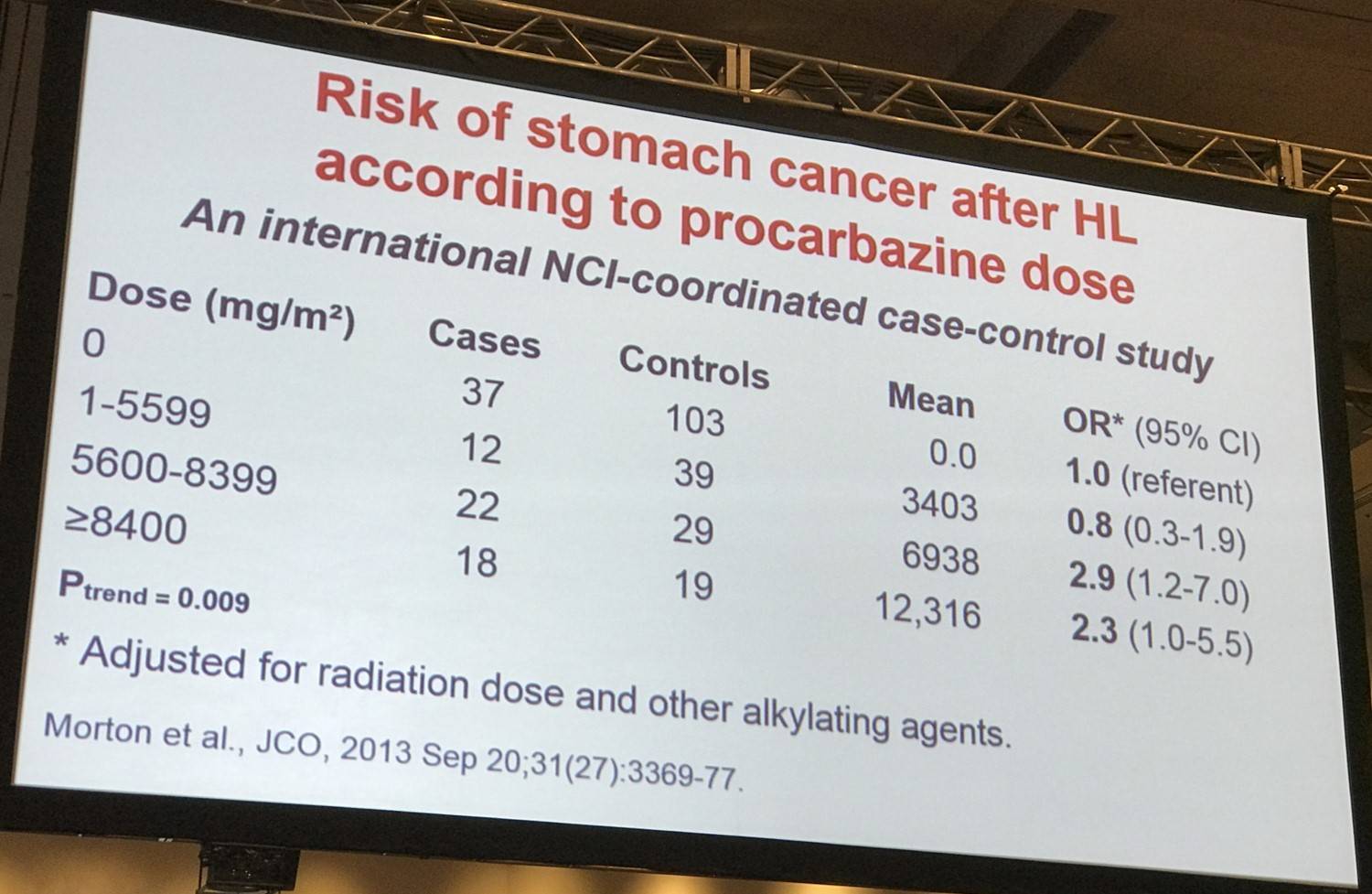
Morton et al. found that stomach cancer risk increased with increasing radiation dose to the stomach (P<.001) and with increasing number of alkylating agent-containing chemotherapy cycles (P<.02). Patients who were administered ≥25Gy radiation to the stomach and ≥5,600mg/m2 procarbazine had significantly higher stomach cancer risk (25 cases; 2 controls; OR, 77.5; 95% CI, 14.7–1452) versus patients who were administered <25Gy radiation and <5,600mg/m2 procarbazine (P<.001).
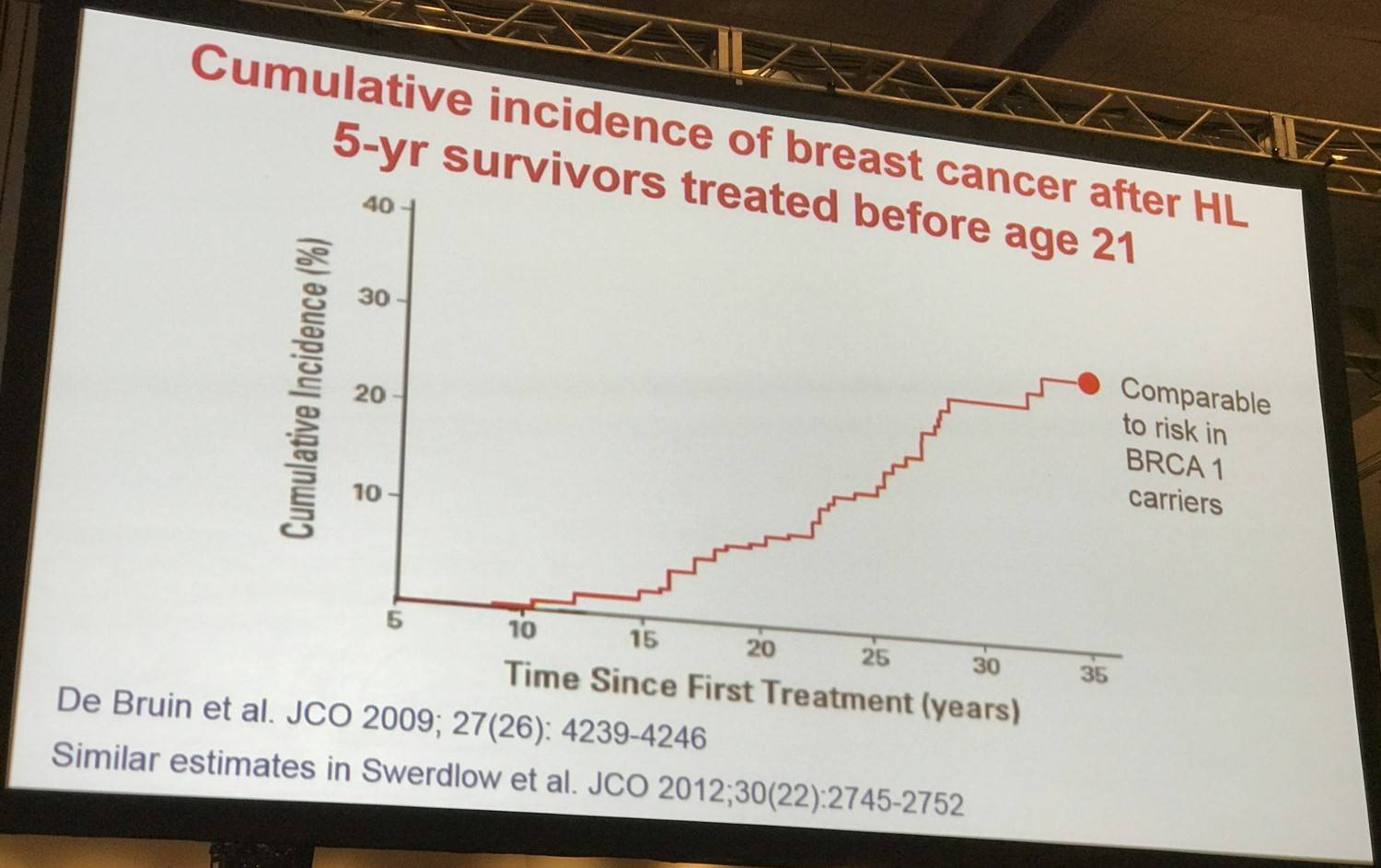
Data published by De Bruin et al. was also shared on cumulative incidence of breast cancer after treatment for HL. The overall cumulative incidence 30 years after treatment was 19% (95% CI, 16–23%); for those treated before the age of 21 years, it was 26% (95% CI, 19–33%).
Van Leeuwen then outlined some potential modifiers of treatment-associated risk of secondary malignancy including age at treatment, genetic factors, smoking, and hormonal factors such as chemotherapy-induced premature menopause. There is much evidence suggesting that early menopause reduces radiation-induced breast cancer risk.
It was then asked why solid tumor risk has not decreased in the recent treatment period? Firstly, there have been favorable and unfavorable treatment changes which have opposite effects on breast cancer risk; less use of mantle field radiation decreases risk yet less use of high dose procarbazine increases risk. Moreover, surveillance has also increased. It is too early yet to observe a decline in second cancer risks due to smaller radiation fields in more recent treatment periods.
Cardiovascular disease
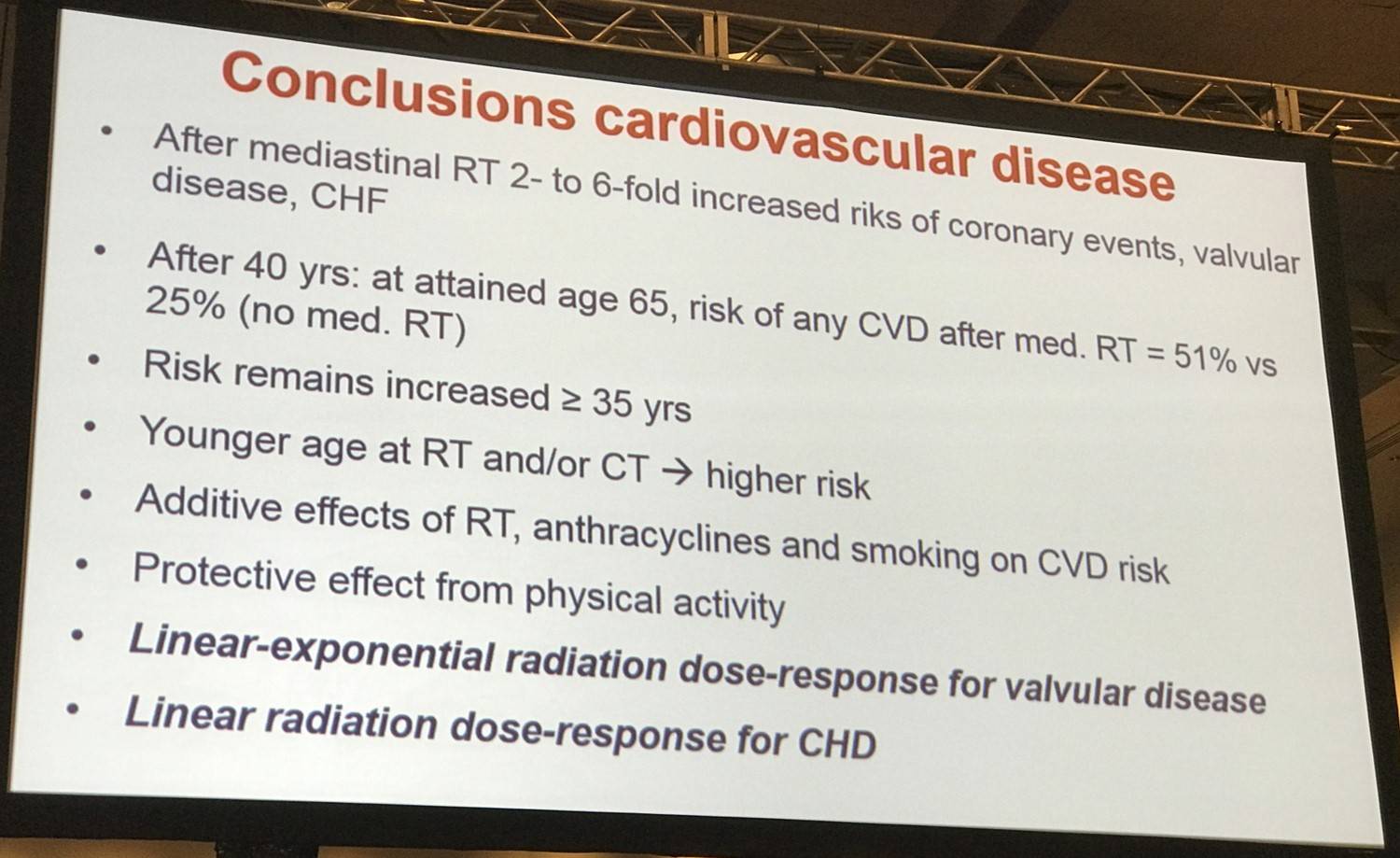
Prof. Van Leeuwen then summarized the findings of a study by F.A. van Nimwegen et al. who published in JAMA Internal Medicine in 2015. They examined relative and absolute excess risk up to 40 years after treatment for HL compared with CVD incidence in the general population and to study treatment-related risk factors for different CVDs. Median follow-up was 20.3 years and was carried out through medical charts and questionnaires to GPs. CVD endpoints included:
- Coronary Heart Disease (CHD), both AP and MI
- Congestive heart failure
- Cardiomyopathy
- Valvular Heart Disease (VHD)
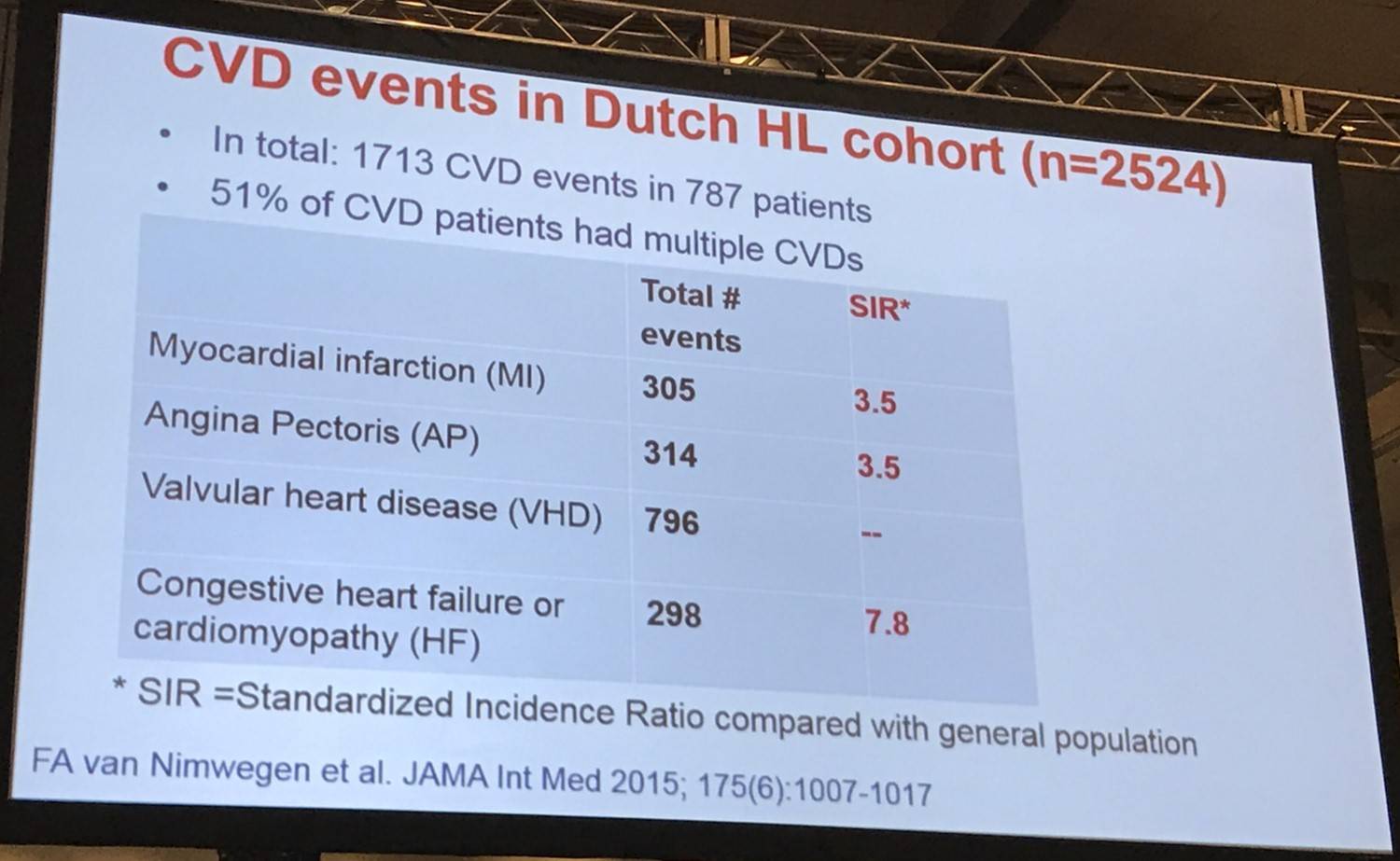
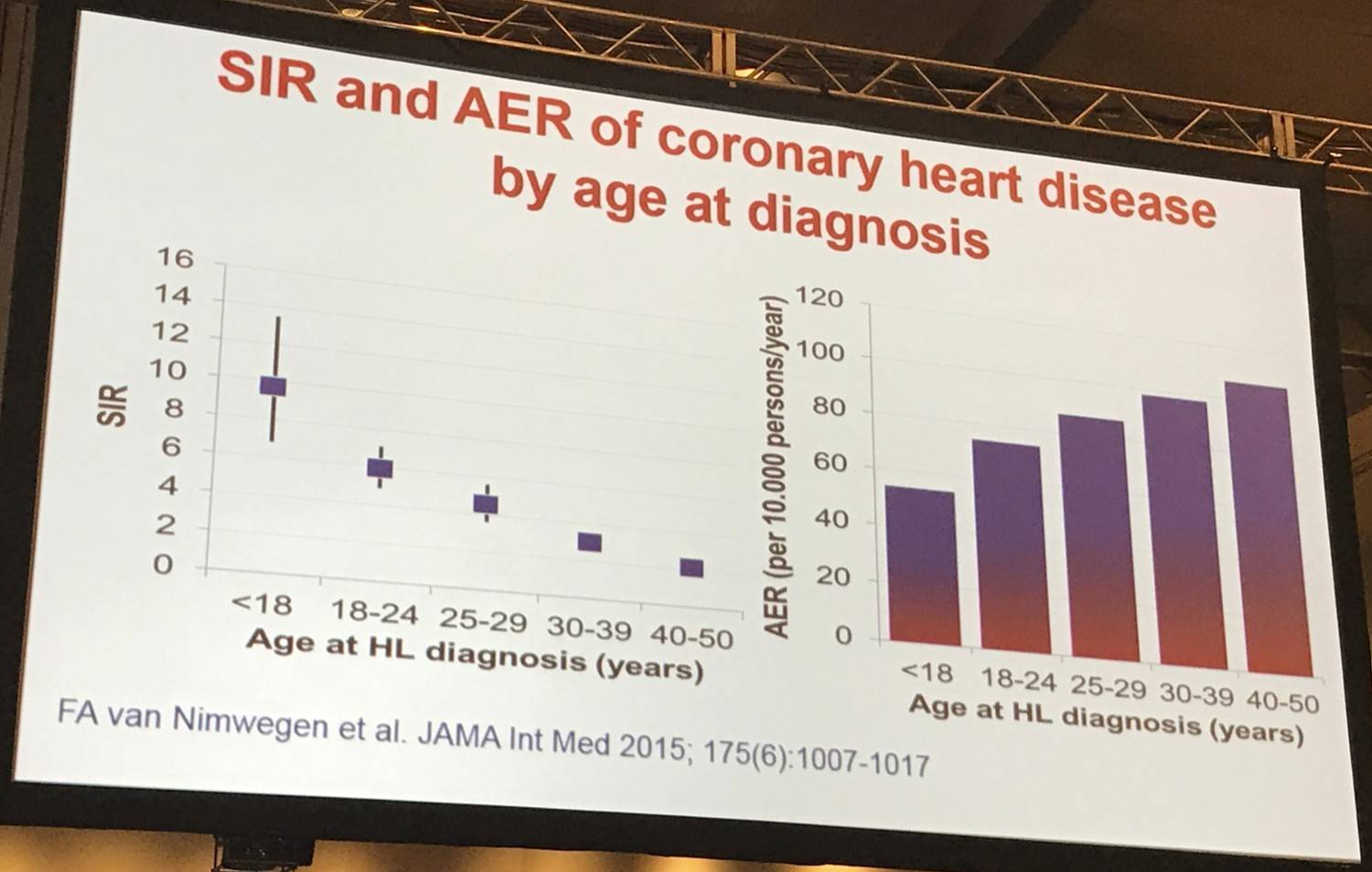
Survivors of HL had a 3.2-fold increased SIR (95% CI, 3.0–3.5) of developing a CHD and a 6.8-fold increased SIR (95% CI, 5.9–7.6) of developing Heart Failure (HF) versus the general population, equating to 70 and 58 excess cases of CHD and HF per 10,000 person-years, respectively. CVD risk did not decrease with longer follow-up and, although SIRs were significantly increased for all age categories, patients treated at a younger age had higher SIRs than patients treated for HL above the age of 35 years.
Mediastinal radiotherapy and anthracycline-containing chemotherapy were associated with increased risk of any CVD (HR for mediastinal radiotherapy, 3.6; 95% CI, 2.8–4.6; HR for anthracycline chemotherapy, 1.5; 95% CI, 1.2–1.8).
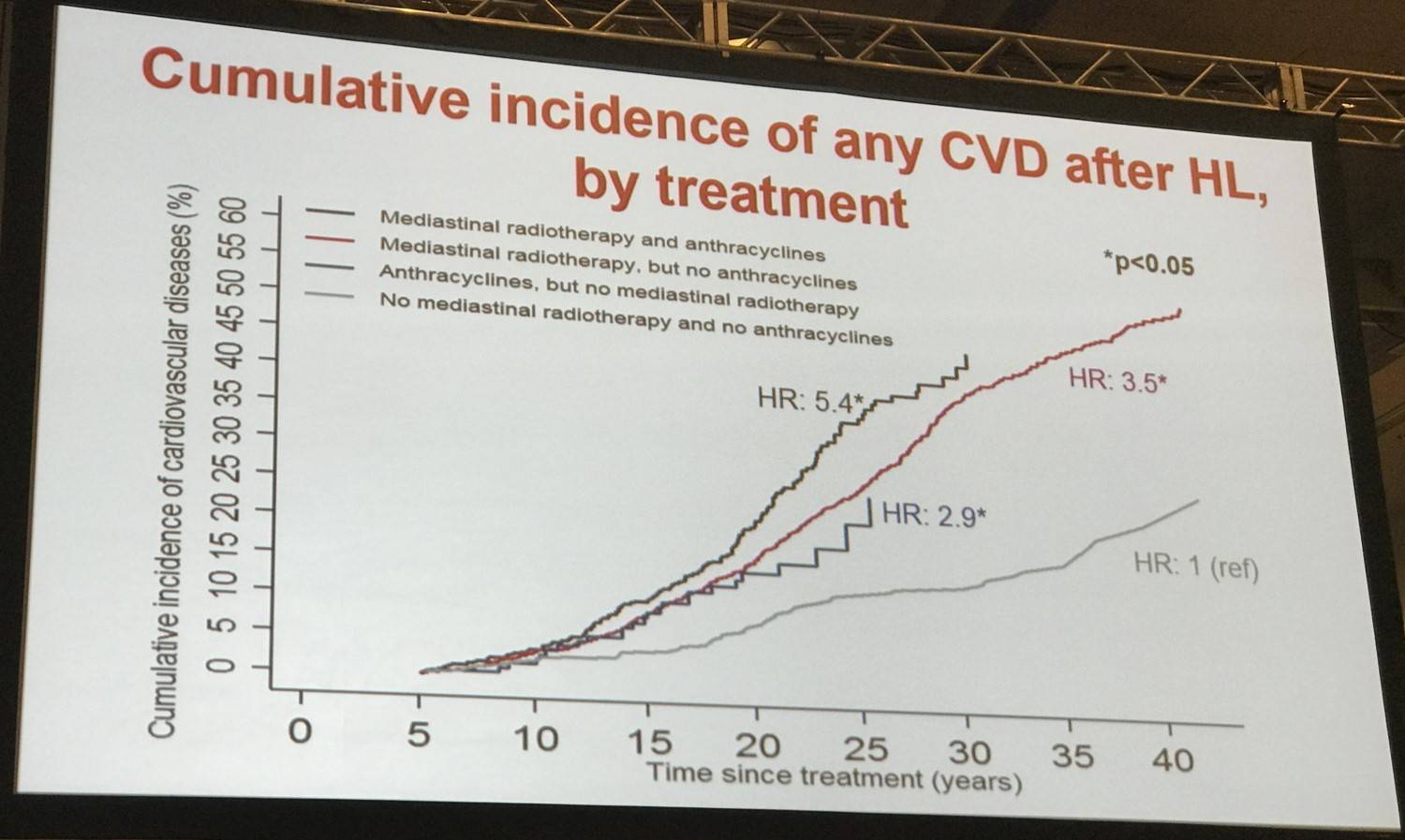
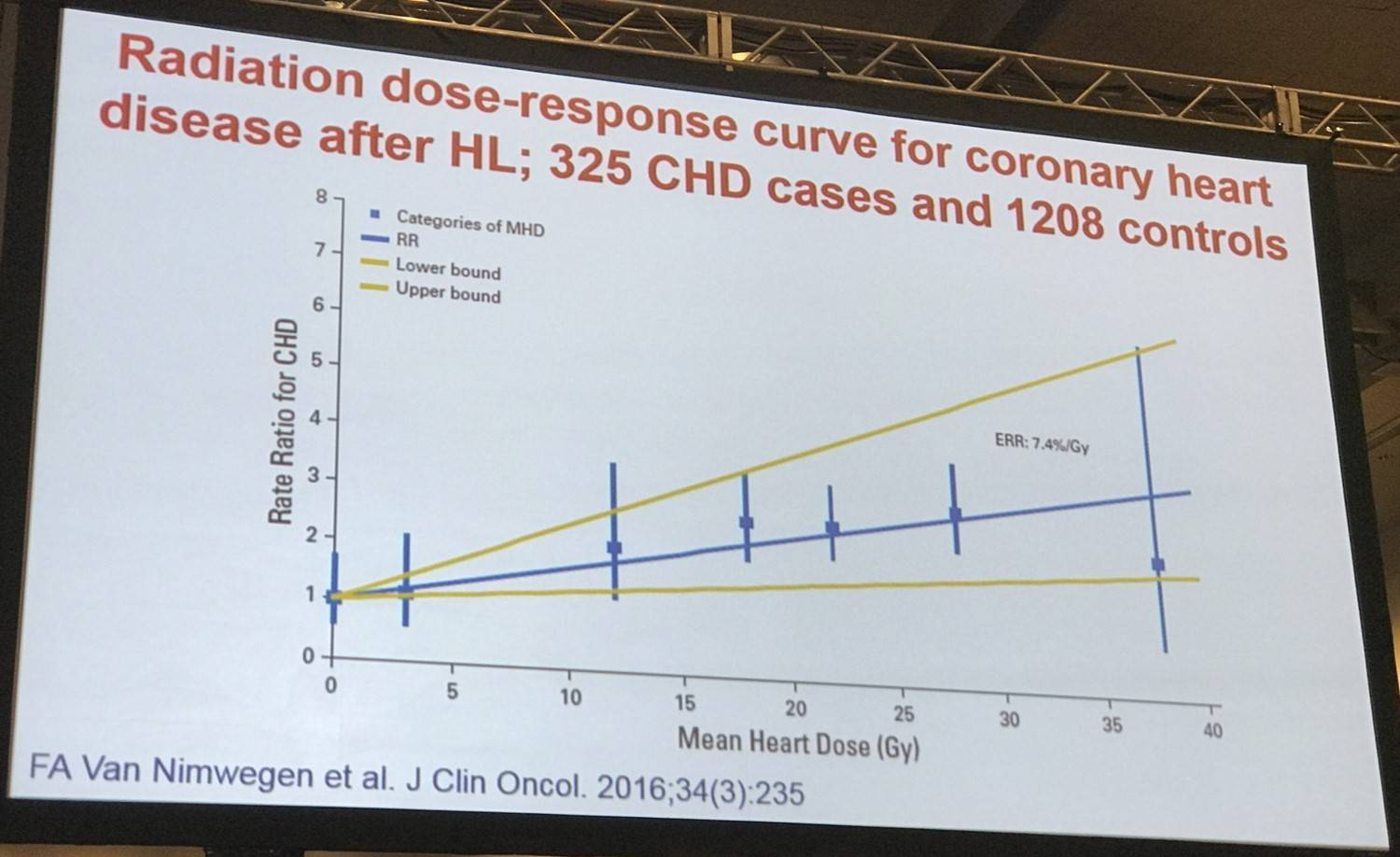
Risk of all CVDs combined and of VHD and HF as first events increased with a higher prescribed mediastinal radiation dose (P = .003, .02, and .03, respectively).
Implications
Prof. Van Leeuwen then outlined some clinical implications for HL survivors and new patients:
|
Survivors |
New patients |
|---|---|
|
Identification of high risk groups for late effects |
Improve risk-adapted treatment |
|
Surveillance when effective screening regimens are available |
Lower volumes and doses of radiotherapy |
|
Dutch BETER project: recalling survivors at high risk |
Lower anthracycline doses (if possible) |
|
|
Prediction models at start of treatment: chances of cure vs late effects |
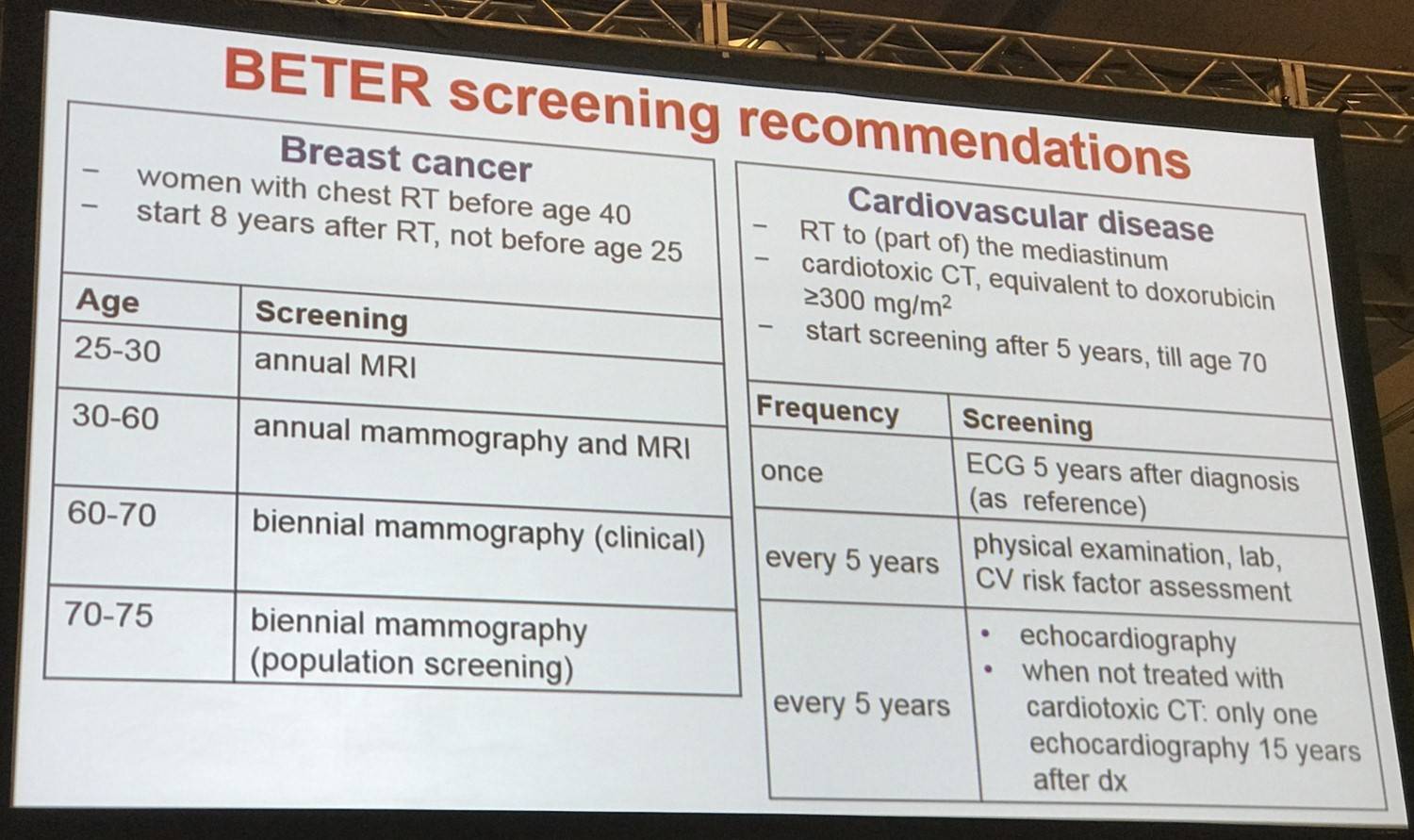
Lastly, screening recommendations from the BETER project were shared. The aim of the BETER HL survivorship initiative was to increase the life expectancy and enhance the quality of life of HL survivors in the Netherlands by reducing the morbidity and mortality from late adverse effects of treatment. 25 hospitals participated in the project.
- Van Leeuwen F.E. Long-Term Risk of Second Malignancy and Cardiovascular Disease After Hodgkin Lymphoma Treatment. 2016 December 3; Educational Session Hodgkin Lymphoma: Treatment Today and the Challenge for Tomorrow. ASH 58th Annual Meeting and Exposition, San Diego, CA.
- Schaapveld M. et al. Second Cancer Risk Up to 40 Years after Treatment for Hodgkin's Lymphoma. N Engl J Med. 2015 Dec 24; 373(26):2499–2511. doi: 10.1056/NEJMoa1505949.
- Eichenauer D.A. et al. Therapy-Related Acute Myeloid Leukemia and Myelodysplastic Syndromes in Patients with Hodgkin Lymphoma: a Report from the German Hodgkin Study Group. Blood. 2014 Jan 29; 123(11):1658–1664. doi: https://doi.org/10.1182/blood-2013-07-512657.
- Morton L.M. et al. Stomach Cancer Risk After Treatment for Hodgkin Lymphoma. J Clin Oncol. 2013 Sep 20; 31(27):3369–3377. doi: 10.1200/JCO.2013.50.6832. Epub 2013 Aug 26.
- De Bruin M.L. et al. Breast Cancer Risk in Female Survivors of Hodgkin's Lymphoma: Lower Risk After Smaller Radiation Volumes. J Clin Oncol. 2009 Sep 10; 27(26):4239–4246. doi: 10.1200/JCO.2008.19.9174. Epub 2009 Aug 10.
- van Nimwegen F.A. et al. Cardiovascular Disease After Hodgkin Lymphoma Treatment: 40-Year Disease Risk. JAMA Int Med. 2015 Jun; 175(6):1007–1017. doi: 10.1001/jamainternmed.2015.1180.

Understanding your specialty helps us to deliver the most relevant and engaging content.
Please spare a moment to share yours.
Please select or type your specialty
 Thank you
Thank youRelated articles
Newsletter
Subscribe to get the best content related to lymphoma & CLL delivered to your inbox